





Original Research
JOURNAL:ACC
 Article Link
Article Link

Diagnosis and Management of MINOCA Patients
Margaret Leslie McDermott, MD, MS
The following are key points to remember from this American Heart Association Scientific Statement on the diagnosis and management of myocardial infarction in the absence of obstructive coronary artery disease (MINOCA):
- 1. MINOCA occurs in 5-6% of acute myocardial infarction (AMI) cases (range reported between 5-15%).
-
- 2. Patients with MINOCA are often younger, more likely to be women, and less likely to have dyslipidemia.
-
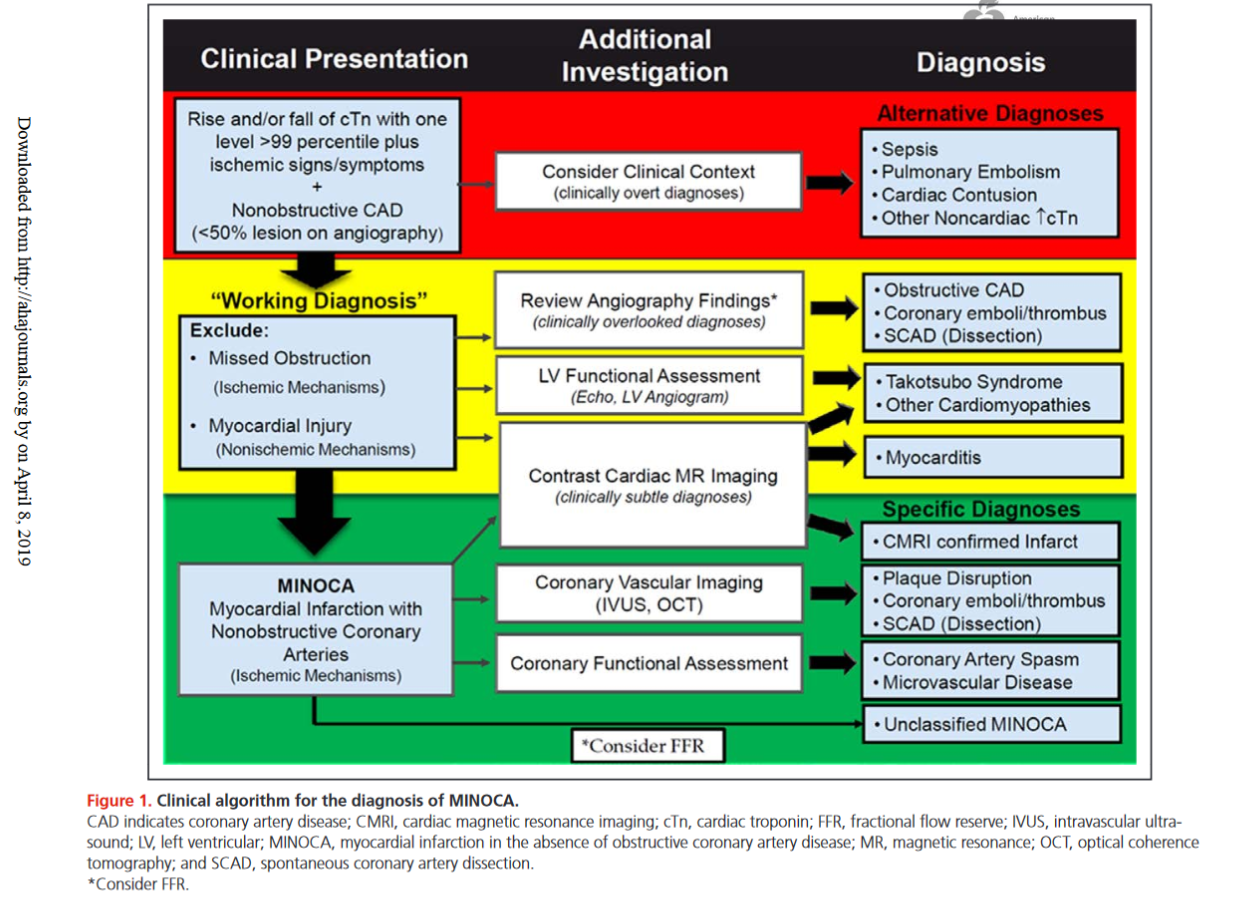
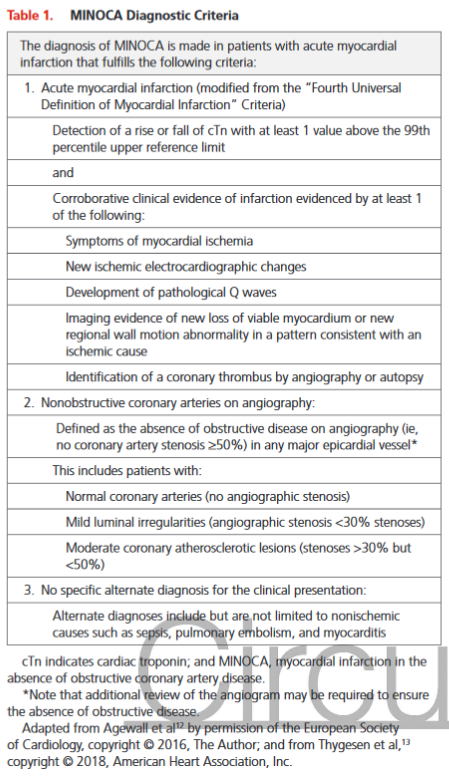
- 3. Diagnosis of MINOCA should be made according to the Fourth Universal Definition of MI, in the absence of obstructive coronary artery disease (CAD) (no lesion ≥50%).
-
- 4. The diagnosis of MINOCA should exclude: 1) other overt causes for elevated troponin (e.g., pulmonary embolism, sepsis, etc.), 2) overlooked obstructive coronary disease (e.g., distal stenosis or occluded small branches), and 3) nonischemic causes for myocyte injury (e.g., myocarditis).
-
- 5. Nonobstructive coronary disease by coronary angiography should be differentiated between patients with normal coronary arteries and minimal luminal irregularities (<30% stenosis) and mild to moderate coronary atherosclerosis (30% to <50%). FFR can be useful. Takotsubo syndrome should be considered separately since it is not considered an MI by the Fourth Universal Definition of MI.
-
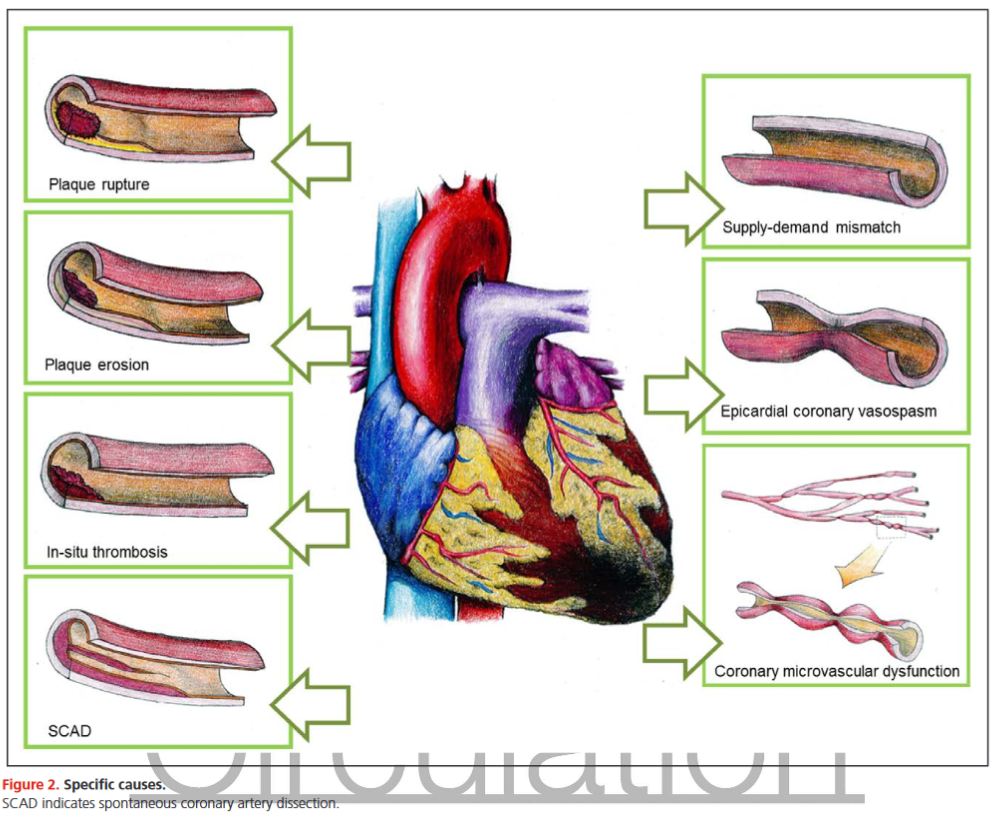
- 6. Plaque disruption is common in MINOCA and encompasses plaque rupture, plaque erosion, and calcific nodules. The authors recommend using optical coherence tomography or intravascular ultrasound imaging in patients with evidence of nonobstructive CAD by angiogram.
-
- 7. Coronary vasospasm is another common cause of MINOCA, defined as >90% vasoconstriction of an epicardial coronary artery resulting in compromised coronary blood flow.
-
- 8. The gold standard technique for diagnosing coronary spasm is administration of high-dose intracoronary acetylcholine boluses with the response evaluated by invasive contrast angiography.
-
- 9. Coronary microvascular dysfunction may contribute to MINOCA and requires further investigation.
-
- 10. Coronary thrombosis or embolism can result in MINOCA, either with or without a hypercoagulable state.
-
- 11. Spontaneous coronary artery dissection (SCAD) should be considered as a cause of MINOCA.
-
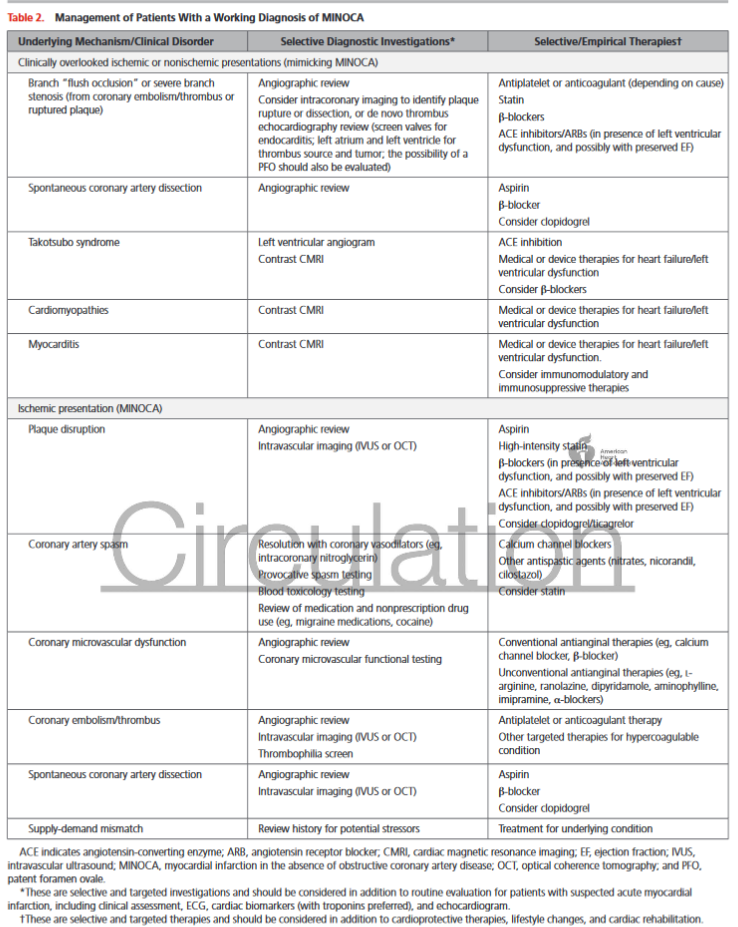
- 12. Management of MINOCA is based on limited evidence and there are no prospective, randomized, controlled trials. Medications (aspirin, statin, beta-blockers, clopidogrel, angiotensin-converting enzyme inhibitors/angiotensin-receptor blockers) should be considered on the basis of the underlying mechanism for MINOCA in each individual. If there is any evidence of atherosclerosis, modifiable CAD risk factors should be treated aggressively.
-
- 13. Coronary vasospasm is best treated with calcium channel blockers, and the benefits of long-acting nitrates are less clear.
-
- 14. Additional research about MINOCA is needed to determine the efficacy of medications aimed at secondary prevention of AMI.

http://www.cbsmd.cn Contact us by cbs@cbsmd.cn
Copyright ⓒ CBSMD Nanjing China. All rights reserved.