





 Article Link
Article Link

Complete Revascularization Versus Culprit Lesion Only in Patients With ST-Segment Elevation Myocardial Infarction and Multivessel Disease
CBSMD
"STEMI patients represent a high-risk patient population that have up to a 50% prevalence of multivessel disease. Consideration of multivessel revascularization in the setting of STEMI may occur in up to one half of STEMI patients. Evaluation of the comorbidities including diabetes, extent of myocardium at risk, lesion complexity, ventricular function, and risk factors for complications such as contrast induced nephropathy which is important in determining the appropriate care pathway." Quoted from Review article "Revascularization Strategies in STEMI with Multivessel Disease: Deciding on Culprit Versus Complete-Ad Hoc or Staged".
Complete or Culprit Lesion Only Revascularization?
the CvLPRIT Trial - "Randomized trial of complete versus lesion-only revascularization in
patients undergoing primary percutaneous coronary intervention for STEMI
and multivessel disease: the CvLPRIT trial"

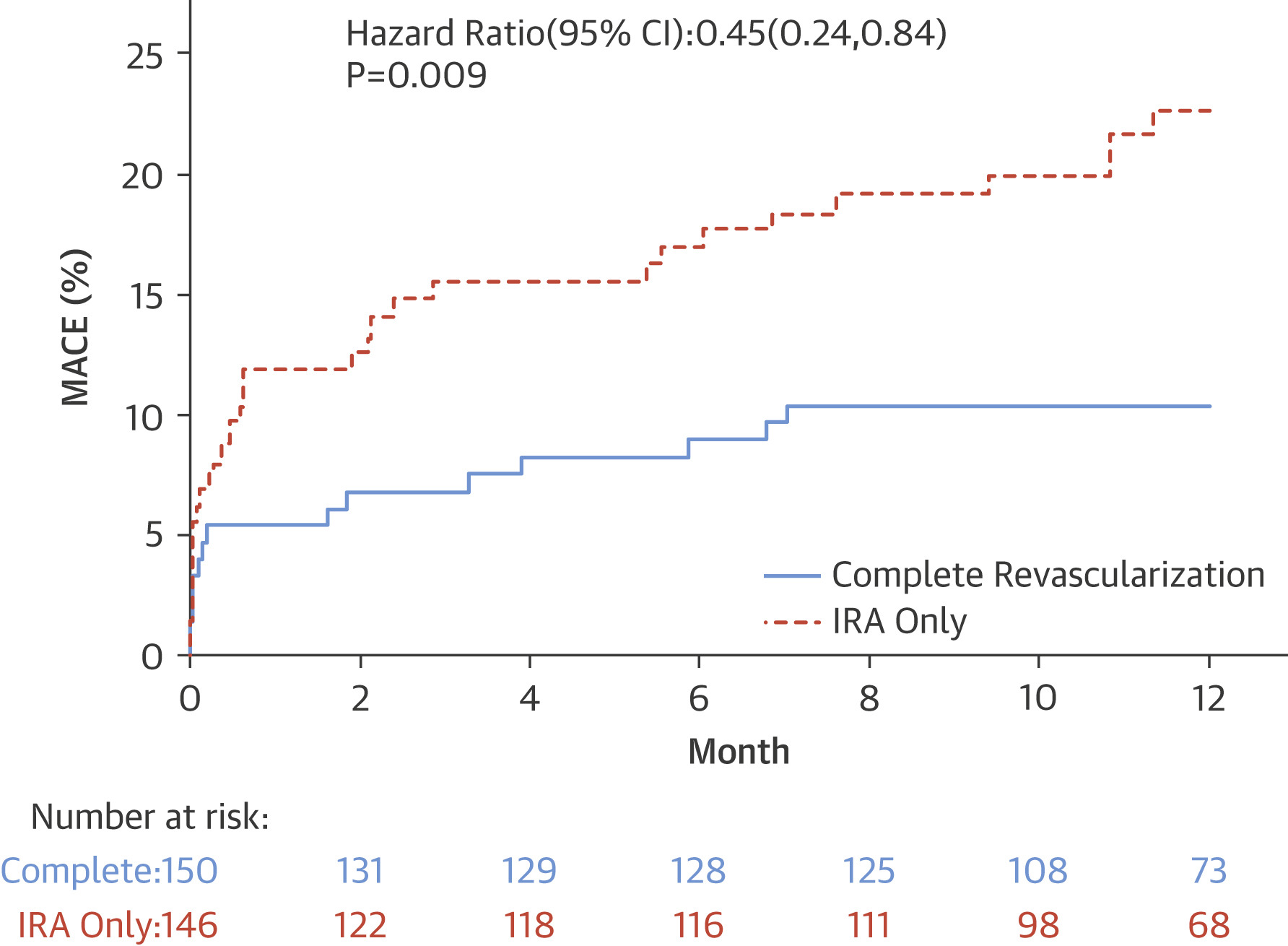
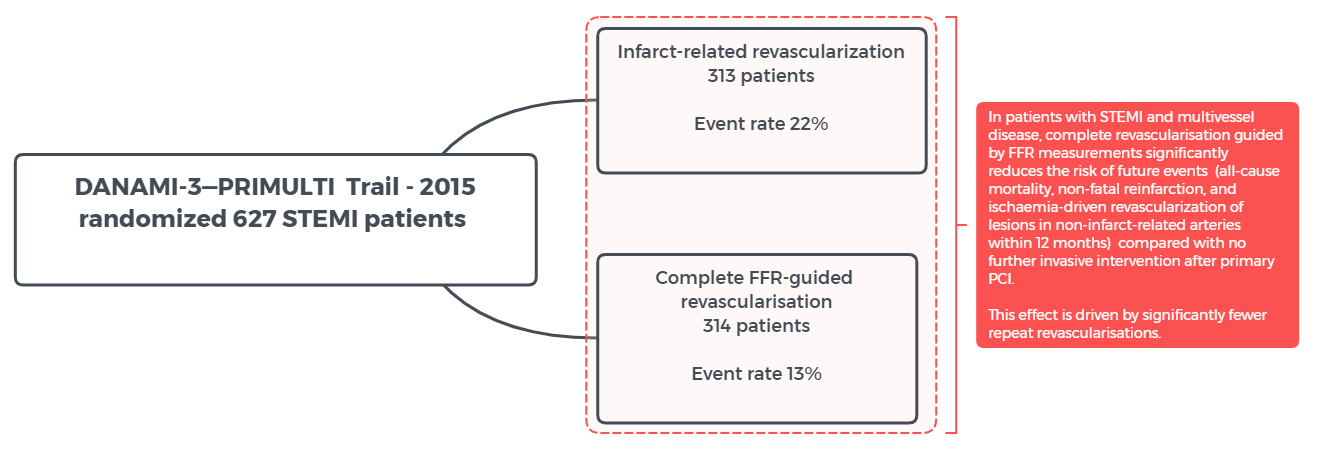
DANAMI-3—PRIMULTI Trial - "Complete revascularisation versus treatment of the culprit lesion only in patients with ST-segment elevation myocardial infarction and multivessel disease (DANAMI-3—PRIMULTI): an open-label, randomised controlled trial"
Compare-Acute Trail - "Fractional Flow Reserve-Guided Multivessel Angioplasty in Myocardial Infarction" concluded "In patients with STEMI and multivessel disease who underwent primary PCI of an infarct-related artery, the addition of FFR-guided complete revascularization of non-infarct-related arteries in the acute setting resulted in a risk of a composite cardiovascular outcome that was lower than the risk among those who were treated for the infarct-related artery only. This finding was mainly supported by a reduction in subsequent revascularizations."
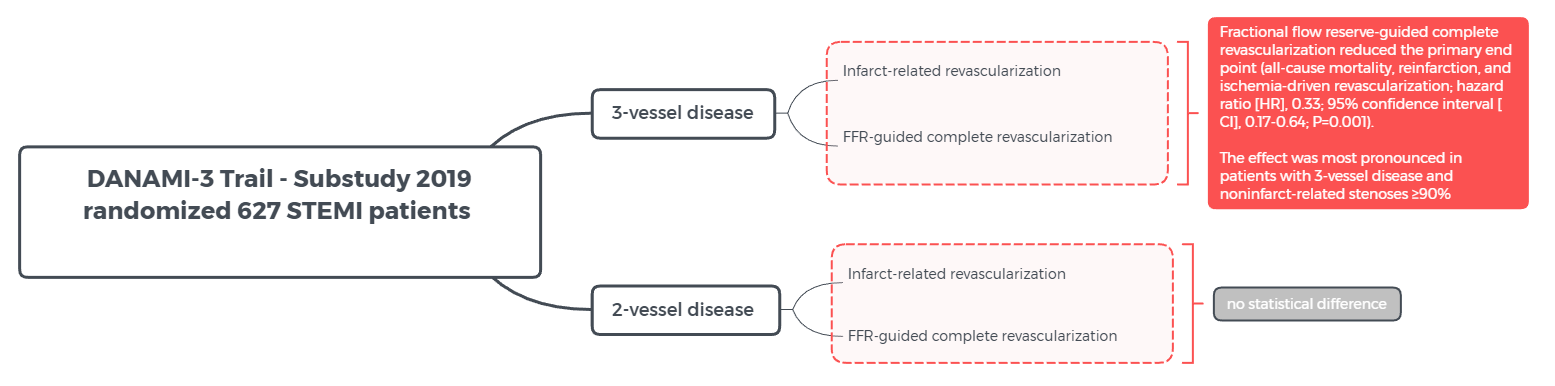
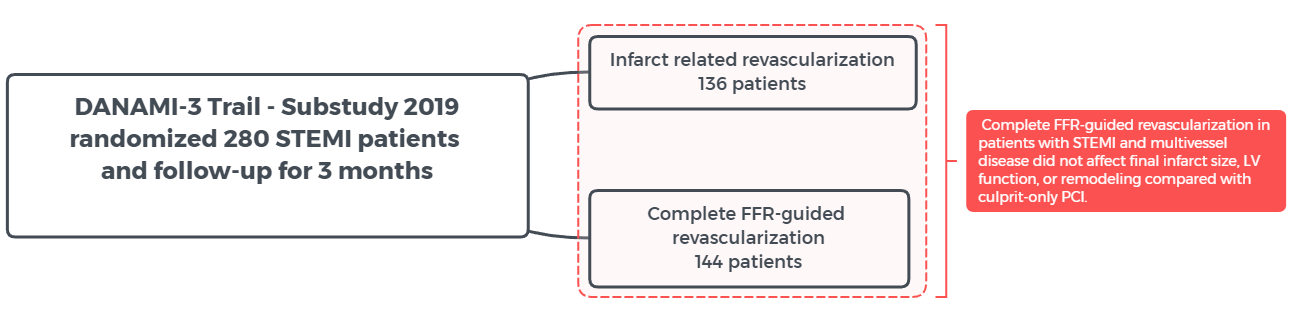
DANAMI 3-PRIMULTI Trial - "Fractional Flow Reserve-Guided Complete Revascularization Improves the Prognosis in Patients With ST-Segment-Elevation Myocardial Infarction and Severe Nonculprit Disease: A DANAMI 3-PRIMULTI Substudy (Primary PCI in Patients With ST-Elevation Myocardial Infarction and Multivessel Disease: Treatment of Culprit Lesion Only or Complete Revascularization)"


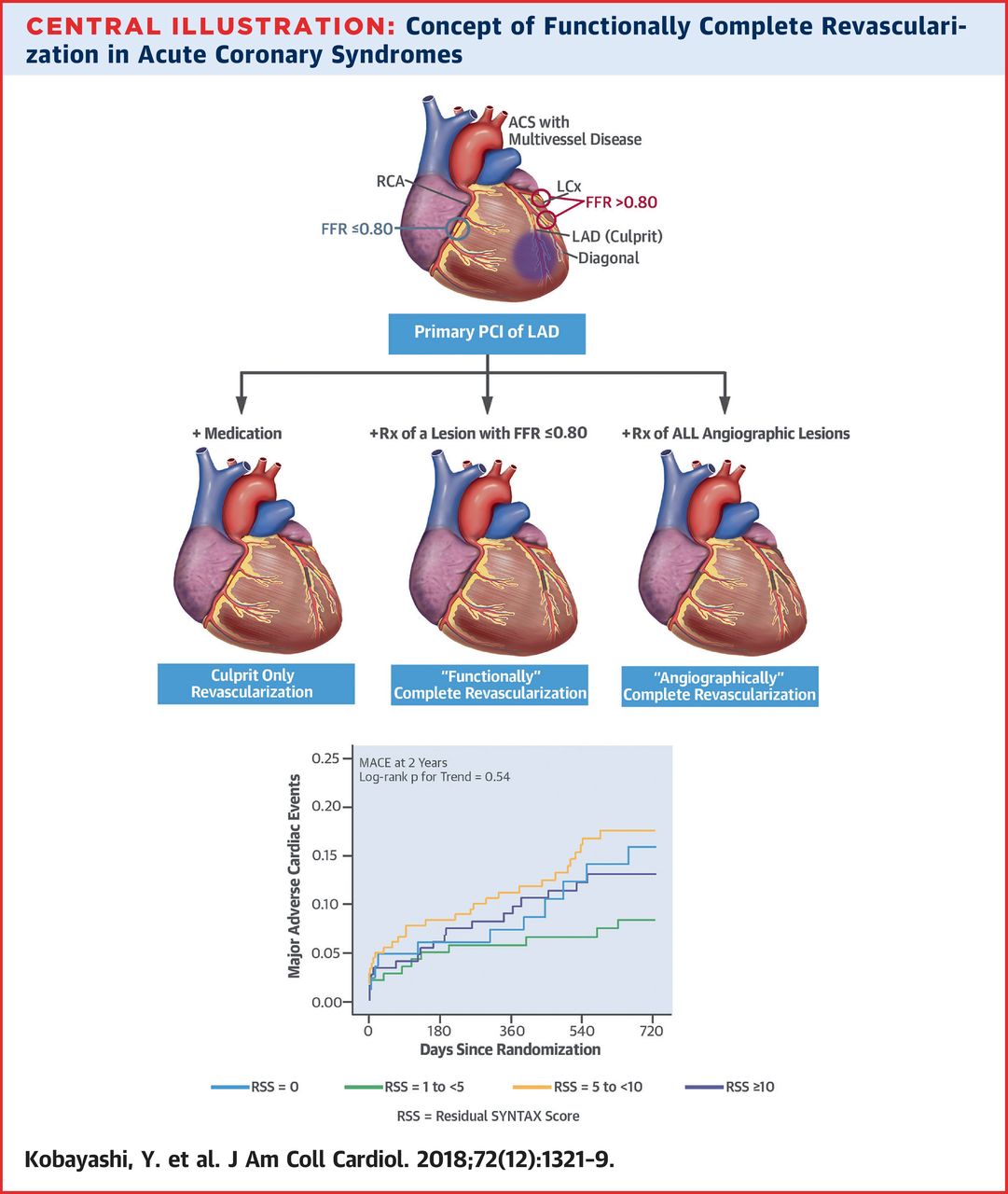
"Prognostic Implication of Functional Incomplete Revascularization and Residual Functional SYNTAX Score in Patients With Coronary Artery Disease" demonstrated that "patients with functional incomplete revascularization showed significantly higher rate of 2-year MACEs than those with functional complete revascularization. A combined anatomic and physiological scoring system (rFSS) after stent implantation better discriminated the risk for adverse events than anatomic or physiological assessment alone.
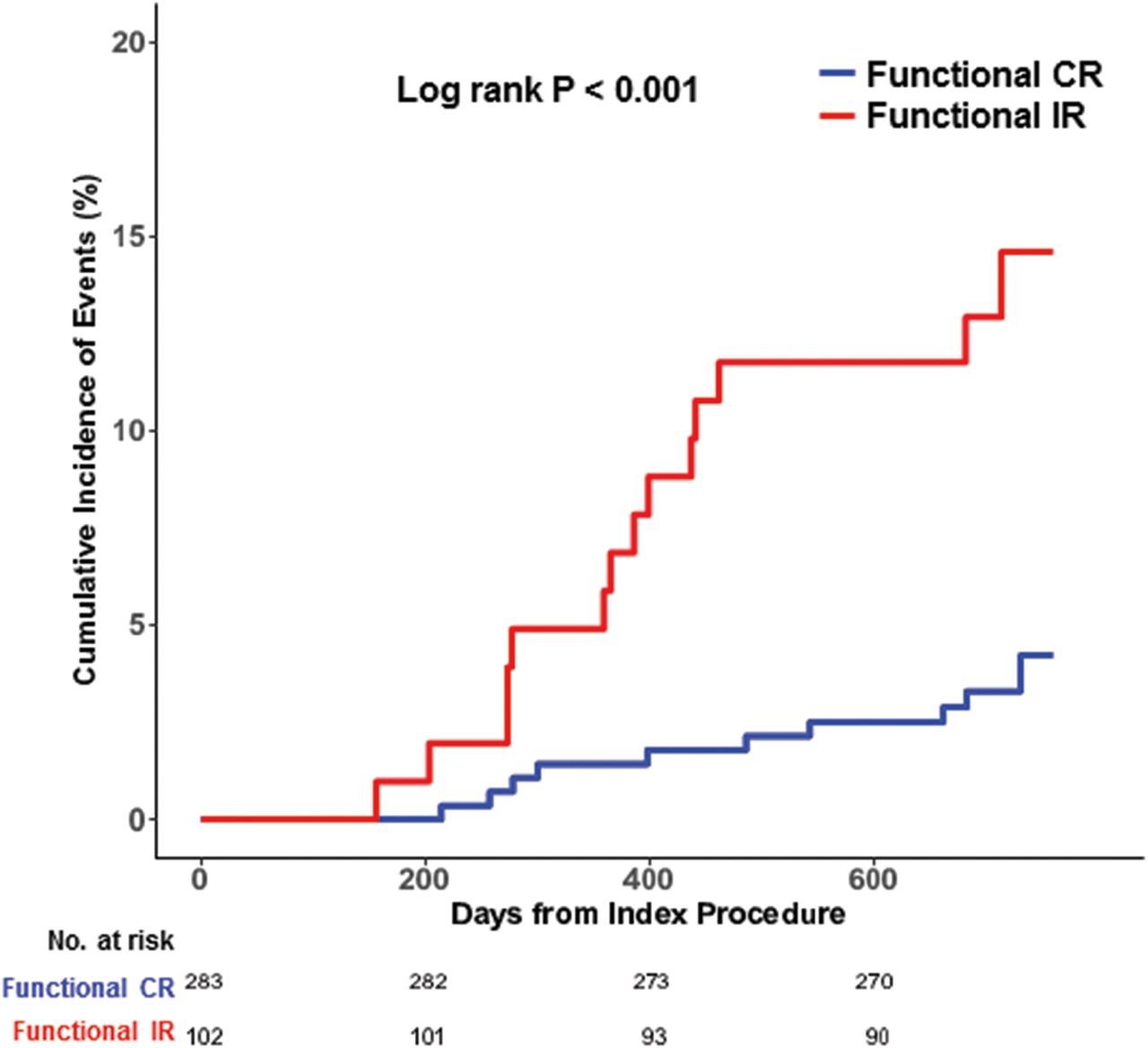
Comparison of 2-Year Clinical Outcomes Between the Functional Complete Revascularization Group and the Functional Incomplete Revascularization Group Kaplan-Meier survival curves are presented for cumulative incidence of 2-year major adverse cardiac events according to functional complete revascularization (CR) and incomplete revascularization (IR) groups.
The COMPLETE trial showed on ESC 2019 that complete revascularization was superior to culprit-only revascularization at reducing death or MI. Among patients with STEMI and multivessel disease undergoing primary PCI, complete revascularization was superior to culprit-only revascularization. Complete revascularization was associated with a reduction in cardiovascular death or MI. This was accomplished without an increase in major bleeding or contrast-induced nephropathy. Previous trials on the topic have demonstrated benefit for complete revascularization, but benefit was mainly due to a reduction in the risk of revascularization. The COMPLETE trial was able to show that complete revascularization was associated with a reduction in ‘hard outcomes’ since the primary outcome was cardiovascular death or MI. In summary, complete revascularization (before or after the index hospitalization) after primary PCI for STEMI is beneficial.

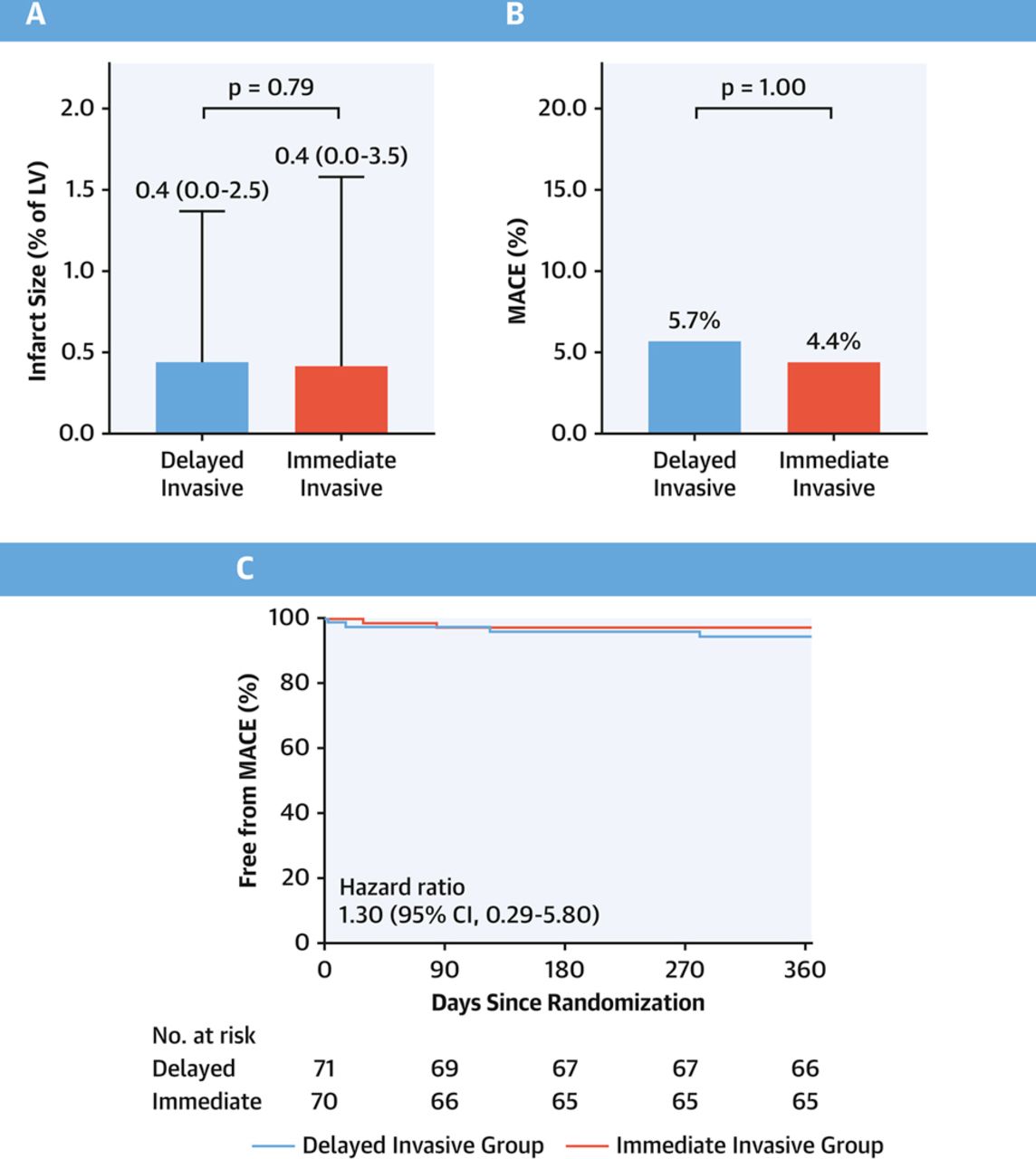
The timing of revascularization had no effect on the final infarct size or the occurrence of major adverse cardiac events (MACE) at one year in patients with transient STEMI, according to follow-up results of the TRANSIENT trial at ESC Congress 2019.

http://www.cbsmd.cn Contact us by cbs@cbsmd.cn
Copyright ⓒ CBSMD Nanjing China. All rights reserved.